

Where does the patient live? That is the first question that doctors have to fill in if they use the European risk model for cardiovascular disease. On The corresponding card Is the Netherlands colored green, Germany yellow and poles orange, just like a few other Central European countries. General practitioner and researcher Janet Kist uses the model in her practice and regularly opts for the Polish category: ‘High risk’, even though her patients do not live in Poland but in a disadvantaged neighborhood in The Hague.
Thanks to that choice, the model recommends intervening faster. For example, someone gets the advice to consider blood pressure or cholesterol lowers faster, or to change their lifestyle. For her patients, often low -income people, that can make the difference between life and death.
Read also
Hindustanis have twice as much chance of a heart disease
Scientific research shows time on time That the risk of heart disease is strongly related to prosperity. Those who are poor have a greater chance of cardiovascular disease. That explains why Poland, a country with relatively low prosperity within Europe, has a ‘high risk’ in the European model. But the model should also take into account wealth of wealth within national borders, says Kist. “For example, if you are forty, you don’t smoke and you have high blood pressure. Then we now tell all those people the same: your risk is low.”
You should say to people with a low income: we know that in your case your risk is actually much higher
That is too general, says Kist. “You should say to people with a low income: we know that in your case your risk is actually much higher. So let’s add something to it. You could grant a multiplication factor, which means that they do not have a 5 percent risk of cardiovascular disease in the next ten years, but 7.5 percent.”
Mortality
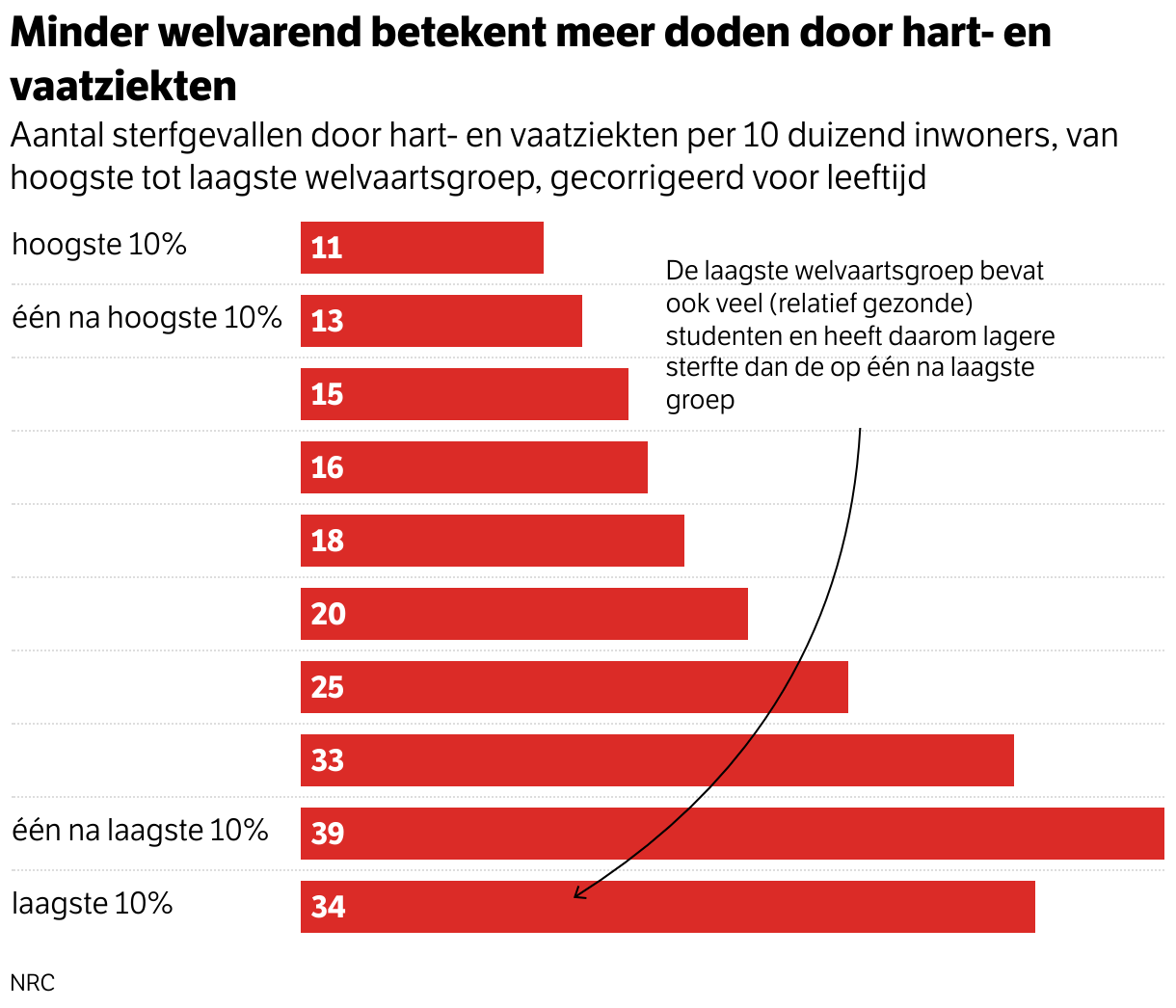
The Central Bureau of Statistics (CBS) published last month A new datasetin which the income and assets of all Dutch people are first linked to the data on mortality due to cardiovascular disease of the same person. The figures show how large the differences are within the Netherlands. Of the people with the highest prosperity, eleven die every year on ten thousand heart complaints. With the lowest welfare group, it is more than 33 deaths, more than three times as much.
When you look locally, inequality is sometimes even bigger says box, which did different analyzes in the province of South Holland. “There we saw differences that run from the lowest Dutch risks to about the level of Poland.” In Poland, 46 of the ten thousand people die from cardiovascular disease every year.
The causes for inequality are largely known. For example, people with a lower socio -economic position have less good access to care. “I regularly have people who only come to me in the consultation room while they do have serious things, or do not want certain studies because they are afraid of extra costs,” says Kist. In addition, lifestyle is an important explanation for the health gap. People with a lower income smoke more, eat healthier and move less.
But, according to Kist, chronic stress also plays an increasing role in the high number of heart problems. “It is pretty complicated in the Netherlands if you are in a lower socio -economic position. You have to request ten different arrangements to get to a normal income. In the past you just received a social assistance benefit. Now you have to apply for your refrigerator, for your children and for your healthcare allowance all request separately. Through the allowance affair that they have to have again and that that they have to have back and that that they have again and that they had to have it again and that that they have again and that they had to have it again and that that they have again and that they have been afraid again and that that they have to have it again and that that they have again and that they had to have back and that that they have to have back and that that they have again and that they have been repaid again and that that they have to have back and that that they have again and that they have been afraid of that.”
Grown
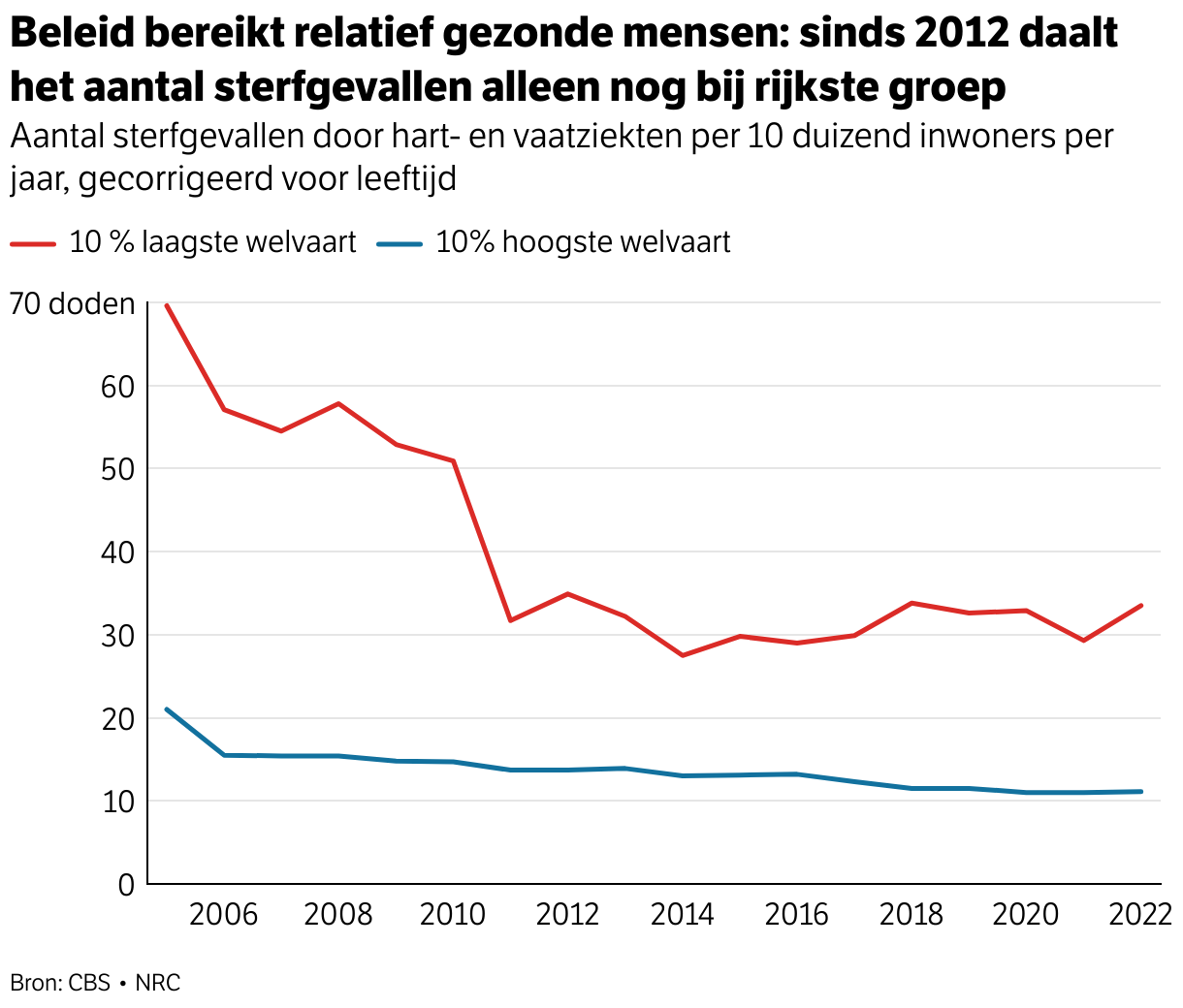
The difference between the poorest and richest Dutch people crumbled for years, but has grown since 2012, according to the figures from CBS. While the number of fatal heart problems among rich people continued to decline, it stagnated for the lowest welfare group. In the meantime, inequality is the same as in 2006.

“There has been a lot of attention for lifestyle in the last ten years,” says Professor of Economy Marike Knoef of Tilburg University. Government measures were mainly focused on food, on sports, on individual behavior. “But you see that it has had an effect on the people who are already relatively healthy. As a result of which the gap between people in high and low lifestyle groups has generally not become smaller.”
Knoef was involved as chairman last year in a cabinet advice of the Social and Economic Council. “One of the main messages was that you should not hamper that individual responsibility so much, but also what the system should do. What does the labor market look like? What does social security look like? What does the living environment look like? They are all very decisive for health.”
The health gap does not only exist with heart disease, but with all kinds of health problems. The 20 percent most prosperous people in the Netherlands therefore live more than eight years longer than the 20 percent least prosperous people. Those who are prosperous also live in good health for 24 years.
Scientists are already doing decades of research To the precise causes for that inequality, the discussion is now increasingly about the solution. That raises fundamental questions about the role of medicine, says Kist. “We, as doctors, cannot solve the inequality. That is not the care. But a part lies with us: should we continue to give equal care in the Netherlands? Or do we have to take a step for people we know they have higher risks?”
Read also
Social class is more decisive for your life than where you live, the SCP says
