
The national social works system, made up of union and management personnel social works, bases its financing on the mandatory contribution of workers.. In the mid-1990s, the principle of captive affiliation to the social work of activity was relaxed, allowing members to choose their social work. This gave rise to the entry of prepaid medicine companies. The implementation was through agreements with social works so that they, in exchange for a commission, would transfer the mandatory contribution to the prepaid.
In 2025, the “derivation of contributions” will end, incorporating prepaid medicine companies into the system to compete directly with social works. The intermediation of the derivative social works was eliminated and people now become direct members of the prepaid ones. As a consequence of this, the system was made up of 290 social works that bring together 64% of the collection and 50 prepaid medicine companies with the remaining 36%. This is an important but specific change that does not solve the most serious financial problems that the system has been accumulating.
In this framework, the main directors of the CGT, in their capacity as administrators of the union social works, issued a “Social Works Situation Report” where they warn about the presence of a systemic crisis that transcends the incorporation of prepaid companies into social security. In this document the CGT points out that:
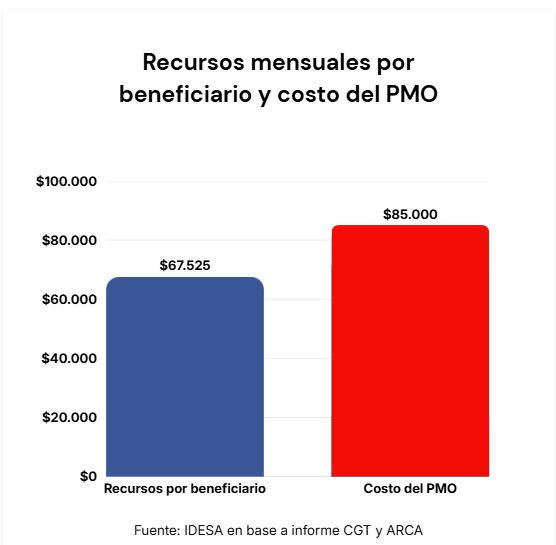
- The average level of per capita resources of the social and prepaid works system is $67,525 per month, data verified with ARCA collection data.
- 67% of affiliates have per capita resources lower than this average.
- The cost of Mandatory Medical Program (PMO) is estimated at $85,000 per month.
These data show that in the social and prepaid work system the available resources are far from covering the costs of the obligations stipulated in the PMO. The dimensions of the lack of financing are magnified when some 2 million monotributistas are counted who were also integrated into the system but who mostly contribute only $22,000 per month. That is, the majority of members contribute below the cost of the PMO.
The PMO was created by a ministerial resolution in 1996 as a list of basic medical benefits. But successive laws expanded it and incorporated non-medical benefits, such as social services for disabilities, addictions and mental health. Likewise, since the list is not exhaustive but open, it is understood that all new innovations in medicine (such as biological medicines) are implicitly included in the PMO. A notable fact is the expansion of the PMO via judicial protections. It is estimated that there is currently 1 protection for every 1,000 members and the trend is increasing.
The basis for beginning to rebuild the system is to reestablish consistency between the benefits that the system is obliged to provide and the financing that is available. To do this, it is essential, on the one hand, to organize the PMO. Social services for disabilities, addictions, mental health, geriatrics must be financed and managed by the State through its competent bodies such as the National Disability Secretariat (ex-ANDIS), Sedronar and the National Directorate of Mental Health. Innovations in medicine must be incorporated, to the extent that they are cost-effective, by the National Commission for Technology Evaluation (CONETEC). In other words, return to the original idea of the PMO as a set of basic and conventional medical benefits. In parallel, it is essential to improve the financing of the 67% of affiliates who are below the average capita. IsIt is possible to use 100% of the Solidarity Redistribution Fund (FSR) to increase the per capita contributions of lower-income families.instead of allocating it to subsidies that the CGT itself recognizes are assigned using arbitrary criteria.
The system of social and prepaid works suffers the consequences of double demagoguery. The first is to incorporate, via laws and judicial rulings, benefits to the PMO without considering its financing. The other is to incorporate people with very limited contributions into the coverage, as is the case of monotributistas. To get out of this deep crisis, it is essential that the promises align with the available financing.
*President of IDESA
by Jorge Colina
Image gallery

![]()
